

(This blog was originally posted here:
http://publichealthy.co.uk/goo...ch-the-case-of-aces/ and on Twitter:
https://twitter.com/andykturne.../1090298657000378369, @andykturner)
-------
Adverse Childhood Experiences (ACEs) are traumatic events that children can be exposed to while growing up. These include the direct impact of suffering abuse or neglect, or the indirect effects of living in a household affected by domestic violence, substance misuse or mental illness. The original ACEs study found that those with a higher number of ACEs were more likely to have physical and mental health difficulties and to engage in health-related risk-taking behaviours than those with less traumatic childhoods. In the 20 years since the study was published the ‘ACEs movement’ has steadily expanded, particularly in the United States.
It took much longer for the first UK ACEs study to be published and it is only really in the last few years that awareness of ACEs has grown on these shores. England is currently lagging behind Wales and Scotland in recognising ACEs in national policy, though many local areas are developing their own ACEs strategies.
I only heard about ACEs two or three few years ago. I was aware of each of the individual experiences that the authors termed ACEs, but not of their being grouped together and counted. There was something about the idea that nagged away at me right from the start, but I couldn’t articulate it. Then I came across a concrete example of good intentions causing harm in a charity I was working alongside. The organisation helps vulnerable people with a range of problems, from domestic violence to involvement with the criminal justice system. Staff had received training on ‘ACE-awareness’ and how to incorporate routine enquiry about ACEs into their work with service users, apparently to offer more tailored support. Many of the staff had faced the same issues as those they were now trying to help, and several reported finding the training distressing. They were told of the potential damage ACEs can cause, which caused them to worry about the impact it had had on themselves. Several reported feeling guilty about having ‘passed on’ their own ACEs to their children. They were taught all about the negative impact of ACEs, but offered no reassurance that you can have a high number of ACEs and still be totally fine. I posted this issue in an online ACES forum and found that it was not an uncommon issue. I’ve since worked on various ACEs projects and think my thoughts are finally just about lined up enough to write down.
There are of course lots of examples of fine work going on around ACEs, but there are also aspects of the ACE movement that make me feel a little uncomfortable. I worry that what is clearly a well-intentioned desire to just do something might not do good and could cause harm. My concerns below are absolutely not meant as a criticism of the motivation and altruism underlying the ACEs movement, but as a cautionary nudge to make sure that, in our enthusiasm to do good, we don’t run before we can walk.
A narrow definition of adversity
The original ACEs study defined ten kinds of adverse experience; five that involved direct harm to a child (physical, sexual and emotional abuse; physical and emotional neglect) and five that affect the environment in which they grow up (domestic violence; substance abuse; mental illness; parental separation; incarceration of a household member). My first thought on reading the paper was – why just these? What about bullying? Hunger? Homelessness? The death of a parent? And why only things that happen within the household, surely community violence is an adverse experience? Since the initial study, a great many others have been published that include one or more of these or other ‘extra’ ACEs. To me this illustrates that, outside of academic research, a focus solely on the ten ‘official’ ACEs was always too narrow.
The ACE movement also seems to conflate adversity with trauma, and the two are very different. In this article, Gary Walsh states that
the term risks suggesting that adversity of any kind is bad or traumatic. While abuse and neglect should always be considered fundamentally wrong, traumatic and preventable, the same cannot always be said for adversity. Everyone will experience adversity at some point and there is often strength and hope to be found in it. Our responses to adversity can nurture resilience and loving relationships while also defining our identities
ACE-awareness
In a way, I think the ACEs movement has become a victim of its own success. It’s in danger of becoming its own distinct field, rather than what I think it should have been: another, powerful piece of evidence to raise awareness of and advocate for what we already knew to be important. It has done that to some extent, of course, but unfortunately it has spawned a distinct campaign that has raised awareness primarily of the ten, narrowly-defined ACEs chosen by the original researchers. The ACEs study provided some excellent population-level data, but I don’t believe it was ground-breaking research. I know to some that might seem blasphemous, but it will not have come as a surprise to anyone that traumatic experiences occurring early in a child’s life can have a lasting impact.
Being ‘ACE-aware’ has become somewhat of a badge of honour. We now have ACE-aware schools, councils, businesses, even an ACE-aware nation. But awareness without action achieves nothing. There is a world of difference between ACE-awareness and trauma-informed practice. The former can mean different things to different people but may mean as little as having heard of ACEs and that they can be harmful. That’s great, but useless on its own. I’m aware of heart surgery, but that doesn’t qualify me to advise a triple bypass. There are of course many examples of people or organisations who rightly see becoming ACE-aware as just one piece of the jigsaw that is effective and comprehensive trauma-informed practice, but plenty of others who believe ACE-awareness is an end in itself; and that can be dangerous, as my earlier example demonstrates.
Medicalisation
There is a great deal of published literature asserting that ACEs can have tangible effects on the biology of individuals. This is powerful stuff and has really helped to raise awareness of ACEs because, rightly or wrongly (well, wrongly), issues are often only taken seriously if they can be labelled as a medical problem or considered a disease. The ACEs movement in the States was, initially at least, led by medics, and that is probably one of the reasons it gained traction.
But… if you think about it, why does it matter if ACEs have demonstrable biological effects? Why does that make the case more powerful? In their submission to the House of Commons Science and Technology Select Committee Inquiry into the evidence-base for early years intervention, Edwards et al. asked what I thought was a really pertinent question:
Would a life lived in the miserable conditions created by adverse situations be wrong even if there were no long-lasting biological effects?
Of course it would. So, while the evidence demonstrating that ACEs have a biological impact has been important in raising awareness, there is a danger that ACEs become yet another example of what is essentially a social issue with societal solutions being labelled as a medical one. When that happens, the focus shifts to identifying and ‘treating’ individuals, rather than prevention at the population level.
Individualism
Time and time again we see the approach to tackling complex social problems focus on searching for ‘solutions’ at an individual level. What that means is that rather than making the necessary but difficult changes to society that would reduce the risk of rubbish stuff happening , we wait for the rubbish stuff to happen then try to mitigate its effect – what Geoffrey Rose called “a targeted rescue operation for vulnerable individuals”. For ACEs, that means that the approach has tended to rely on finding individuals with a high ‘ACE score’ and then trying to help them (a bit more on the ACE score and that assumption of needing help later). It’s a natural and intuitive approach to medicine, but we also know from Rose that, on its own, it has little effect at the population level. For pretty much any disease or negative outcome you can think of, the greatest burden will fall on the vast majority of people considered as low-risk, simply because of their greater numbers:

If we want to prevent ACEs and their consequences at a large scale, then a population approach where we shift the level of risk in the entire population is required. For that we need to prevent the causes of ACEs, and not only act on those individuals already affected. Really, of course, we need to both offer targeted help to those that need it and reduce the level of risk in the whole population (Rose called these the ‘high risk’ and ‘population’ strategies, respectively). But we’re all skint because of funding cuts, and we can’t do both. We’re forced to choose between helping those in most pressing need or incrementally improving population health. In that situation, the former always wins. But what a shame we’re forced to choose.
ACE scores, screening and ‘routine enquiry’
The ACE score (i.e. the number of ACEs an individual has experienced) was designed for population-level epidemiological research. It was not intended to inform practice at the individual level. In their final report, the Science and Technology Committee explicitly state that “the simplicity of [the ACEs] framework and the non-deterministic impact of ACEs mean that it should not be used to guide the support offered to specific individuals.”
Demonstrating an association (note association, not cause) between high numbers of ACEs and poor outcomes at the population level tells us precisely nothing about any individual with a high ACE score. It is absolutely possible to have ten ACEs and be total fine, or to have no ACEs and be a gibbering wreck (I’m proof of that). It is the very definition of an ecological fallacy, yet many advocate its use as a screening tool.
A short while ago I attended a meeting for an organisation who were conducting some research into the experiences of young people involved with the youth justice service. When they passed around the questionnaire they’d been using, I was shocked to see they were asking questions about ACEs. To children. When I asked why they were asking them, they were unsure. They had no plan for what to do with the information and hadn’t thought about whether it might be upsetting. The questionnaire was being administered by an 18 year old girl with no training. Luckily, following advice from myself and others, they removed these questions.
There was absolutely no malice in what they were doing of course, they were acting with the best intentions and, well, being ACE-aware I suppose. But any form of screening has the potential to do more harm than good and we “shouldn’t let good intentions undermine […] screening principles”. Screening for ACEs risks labelling individuals who are otherwise content and well and basically fine, or signposting them to services they don’t need. Or, perhaps worse, highlighting issues that need urgently addressing, but not knowing how to. This paper by David Finkelhor cautions against prematurely screening for ACEs and is a must-read. He states that we don’t yet have any evidence-based interventions for high ACE scores and we don’t understand the potential negative outcomes and costs of screening:
if general ACE screening were to result in a big increase in unnecessary and inherently expensive child welfare referrals and investigations as one of its main outcomes, we might look back on the ACE mobilization as a disastrous distraction to the development of evidence based child welfare policy
I’ve also come across advocates for ‘Routine Enquiry for Adversity in Childhood’. “It’s not screening!”, they say. It is screening. There is no evidence it has a positive effect on outcomes. When I’ve raised this I’ve been pointed to this evaluation as evidence. In fact, it states that:
- None of the sites successfully implemented the REACh program
- “One of the underlying assumptions […] is that the enquiry process itself may be therapeutic” but that “practitioners raised concerns that this may not be the case”
- “Concerns were expressed around the ethics of identifying ACEs without the ability to offer appropriate support to those who may need it”
- “Little evidence currently exists on the value of routine enquiry about childhood adversity, using the ACE (or equivalent) questionnaire, or the responses or interventions required for those reporting childhood adversities”
So not really evidence of effectiveness, then… and yet it’s been rolled out across several services in England, including the charity I spoke of in my example earlier.
ACEs as a cause
There is no doubt a strong correlation between ACEs and negative outcomes in no longer life, but that does not necessarily demonstrate causation (see Correlation and causation in the Committee report). I think of ACEs as a symptom of an underlying cause: shit life syndrome, basically. I think this is illustrated really well by the Building Community Resilience (BCR) ‘pair of ACEs’ framework:
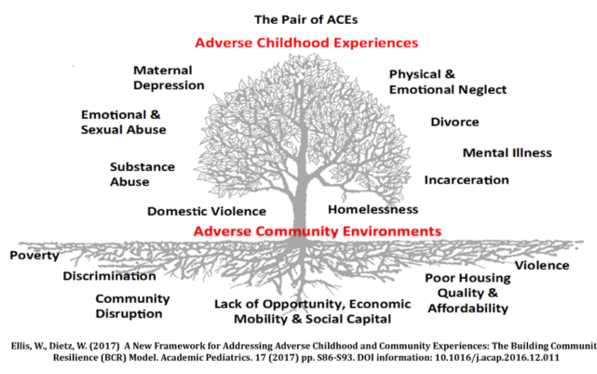
The Pair of ACEs Tree demonstrates the interconnectedness social circumstances and adverse experiences of their family environment. The leaves on the tree represent the ‘symptoms’ that are easily recognized in clinical, educational and social service settings, but the underlying causes are the usual suspects: a lack of affordable and safe housing, community violence, inequality, discrimination, poverty, etc..
If difficult lives (or ‘adverse socioeconomic circumstances’) are the root cause of ACEs, then I’m not sure we even need distinct ACEs prevention strategies; it’s the same as preventing everything else. What we need is the funding and freedom to develop broad prevention approaches that focus upstream. A living wage. Clean streets. Good, affordable housing. Parks. Stuff for teenagers to do. Welfare. Jobs. Childcare. Good schools. Of course, we could never prevent everything, so we will always need access to excellent individual support. But that is not going to reduce the incidence. Trauma-informed practice and proper help for individuals is absolutely essential, but it’s not really prevention is it? We need to tackle the roots of the problem too.
Summary
I’ve banged on for ages here, so I want to just reiterate that I know there are many hundreds of people and organisations doing excellent, holistic work on ACEs, and that much of what I’ve written will not be new or relevant to them.
But I have witnessed practices being adopted that aren’t (at least yet) based on evidence, but rather the very human desire to just ‘do something’ to alleviate a perceived injustice. Public health is an evidence-based discipline, but we are all human. We will at times be guilty of picking evidence to suit our own narrative, even unconsciously and with the best intentions. If something seems important, we may choose to do it quickly rather than do it properly. It’s not just ACEs of course: MECC, social prescribing, apps…. all being rolled out without robust evidence, all ignoring upstream factors to a greater or lesser extent. It’s something we need to be a little wary of more generally and be careful not to run before we can walk. ACEs are no doubt an important advocacy tool that reflect deeper, underlying problems; but we must not lose sight of the bigger context and wider determinants of public health issues.
Other (better) critiques of ACEs
Much cleverer people have written much more eloquently than me about these issues. I’ve found those below useful – all very worth a read.
- Edwards et al. (2017). The problem with ‘ACEs’: EY10039: Submission to the House of Commons Science and Technology Select Committee Inquiry into the evidence-base for early years intervention. A very robust criticism of the ACEs approach, which garnered strong support in response from a number of other academics similarly concerned about the limitations of the ACEs approach.
- Finkelhor (2017). Screening for adverse childhood experiences (ACEs): Cautions and suggestions. Child Abuse and Neglect.
- Taylor-Robinson et al. (2018). Adverse childhood experiences or adverse childhood socioeconomic conditions? The Lancet Public Health.
- The Times Educational Supplement has published several articles arguing for and against the ACEs movement:
- Barrett (2018). Why I worry about the ACE-aware movement’s impact.
- Zeedyk (2018). Childhood trauma: Why I celebrate the ACE-aware movement’s impact.
- Walsh (2018). The ACEs campaign: cause for worry or celebration?
Comments (13)