
When the Association of State and Territorial Health Organizations (ASTHO) fielded the ACEs capacity assessment tool (ACECAT) in 2019, it prompted a 75% response rate, reflecting the states’ growing awareness of the impact of ACEs on health and eagerness to add to the body of knowledge about states’ activities and capacities around ACEs. After participating in the ACECAT, Nicole Daley, Director of the Massachusetts Department of Public Health’s Division of Violence and Injury Prevention, told ACEs Connection that the survey added to the department’s awareness of the impact of ACEs. Daley later became the Principal Investigator for the CDC Preventing ACEs: Data to Action (PACE-Data2A) grant program.
ASTHO’s focus on ACEs—particularly on how to prevent them—has been significant, especially over the last several years. ASTHO says it and its members are committed to reducing ACEs “to improve long-term health, access to life opportunities, and the overall health of Americans.” This position is summarized in a two-page brief issued in February, 2019 entitled “Adverse Childhood Experiences: Primary Prevention.” Another publication, Data-Driven Primary Prevention Strategies for Adverse Childhood Experiences, builds on this brief.
ASTHO also issued the Preventing ACEs Framework with the purpose “to provide state and territorial health agency leadership (S/THA) concrete resources and examples of how to impact system levers to advance ACEs prevention. Resources are comprehensively organized into five main system levers: data, policy, financing, messaging, and cross-sector partnerships.”
Both as a funder and partner, the Centers for Disease Control and Prevention (CDC) supports the ACEs work of ASTHO, including the ACEs Learning Community. The findings and recommendations contained in the CDC document, the 2019 Preventing ACEs: Leveraging the Best Available Evidence, are consistent with ASTHO’s ACEs priorities.
ACEs LEARNING COMMUNITY
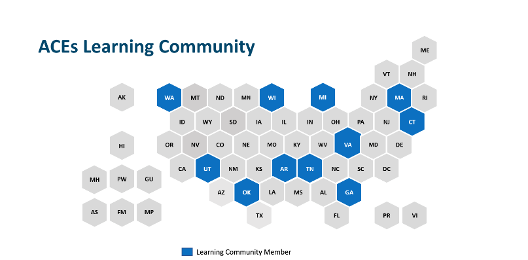
Eleven states are now involved in the ASTHO ACEs Learning Community that aims “to promote cross-sector collaboration to advance the primary prevention of ACEs.” Four of the eleven states (GA, CT, MA, and MI) are participants in CDC’s Preventing ACEs: Data to Action (PACE-Data2A) program. The goals of the Learning Community include:
—Promote cross-section collaboration
—Support state peer learning and relationship building opportunities to identify evidence-based and experience-based practice
—Develop tools and resources to promote to the primary prevention of ACEs and bridge the connection of ACEs to substance misuse, suicide, and violence prevention.
The four PACE-Data2A states will choose technical assistance options from a menu that addresses policy, cross collaboration, data to action planning and other issues.
ACEs CAPACITY ASSESSMENT TOOL (ACECAT)
On January 21, ASTHO released a series of infographics based on the findings of the ACEs Capacity Assessment Tool (ACECAT) survey that was designed to document the capacity of state and territorial health agencies (S/THA) to prevent and mitigate ACEs. The survey asked how ACEs work is being funded and conceptualized at the state level and how sectors are collaborating. The survey was sent to all 59 member agencies. The data are cumulative and do not identify specific responses by agency.
The ACECAT infographics are organized in three general topic areas: 1) Priorities related to primary prevention of ACEs; 2) Opportunity for state and territorial health agencies to improve health equity and ACE disparities; and 3) Strengths of health agencies and partnerships. Each infographic includes a closing section entitled “Looking Forward” that includes key recommendations.
Primary prevention
The survey found that 15 S/THAs are prioritizing primary prevention strategies that prevent ACEs from occurring in the first place; 10 S/THAs are prioritizing infrastructure strategies; 9 are prioritizing secondary prevention strategies that identify high-risk populations; and 5 are prioritizing tertiary prevention strategies that mitigate long-term harm.
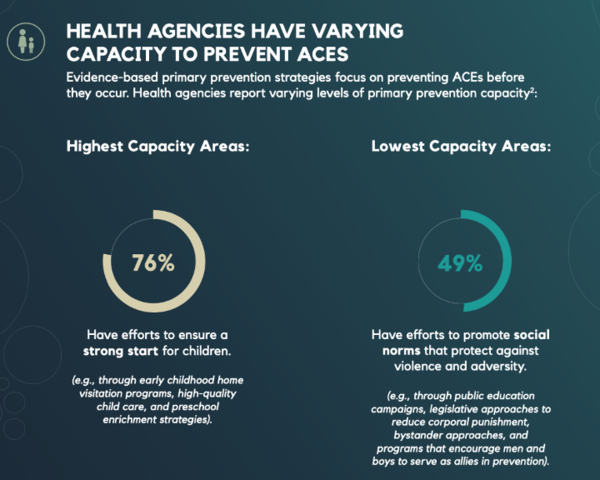
S/THAs were found to have varying capacity to prevent ACEs before they occur. The highest capacity areas (76%) have efforts to ensure a strong start for children. These efforts include early childhood home visitation programs, high-quality child care, and preschool enrichment strategies. The lowest capacity areas (49%) have efforts to promote social norms that protect against violence and adversity. Examples of these efforts include vehicles such as public education campaigns, legislative approaches to reduce corporal punishment, bystander approaches, and programs that encourage men and boys to serve as allies in prevention.
Other high capacity areas include S/THA’s efforts to teach youth new skills to manage stress, conflicts, and emotions (76%) and have interventions to lessen immediate and long-term harms of ACEs exposures (56%). Other low capacity areas include S/THA’s efforts to connect youth to caring adults who are positive role models (46%) and that are working to strengthen economic supports to families through financial security and family-friendly work policies (34%).
Capacity areas are sourced from the 2019 CDC document “Preventing Adverse Childhood Experiences (ACEs): Leveraging the Best Available Evidence.”
Looking forward: Cross-sector partnerships can be used to create programs with a large societal impact. Health agencies should continue to focus on promoting social norms, connecting youth to caring adults and activities, and strengthening economic supports to families.
Health Equity and ACEs Disparities Data
The survey found that health agencies need to enhance surveillance systems to reduce ACEs. Just over half (54%) of agencies have identified high-risk populations, assessed their needs, and created targeted initiatives to address them. ASTHO reports that fewer departments reported the capacity to identify populations with high ACE burden. The survey found that health agencies are monitoring high-risk communities at the following rates:
—Foster care children (47%)
—Communities experiencing concentrated poverty (36%)
—Communities experiencing concentrated violence (25%)
—Juvenile justice and its involved populations (22%)
Of the capacity items measured, the lowest activity measured was health agencies work with correctional agencies to support children of incarcerated parents. ASHTO states that “health agencies can strengthen supports for children with incarcerated parents and juvenile justice populations to stop the cycle of incarceration.” A striking 89% of health agencies have no or limited capacity to work with correctional agencies and only 23% work with juvenile justice systems and their involved populations.
ASTHO identifies two areas where agencies can enhance support for children by improving efforts in two areas: utilize law enforcement data (just 37% of agencies do this) and promote strategies in which first responders link children affected by parental loss to care (29% of agencies have strategies in this area).
This infographic states that “Health agencies need to move to transformational approaches” that work to drive change on a large-scale, societal level as opposed to transactional approaches that “are grounded in reciprocity and navigating existing structures.”
Looking Forward: The ACECAT results reveal gaps in surveillance system data, partnerships with justice systems, working with high ACE-burden populations. Incarceration and familial separations can have negative impacts that impede a family’s ability to offer a safe, stable, nurturing environment that children need to thrive. Health agencies can use these ACEs prevention strategies to make an impact.
Partnerships
Health agencies report partnerships with public and public-private sectors to prevent ACEs at some or full capacity: 76% have partnership with public sector partners and 68% have public-private partnerships. Almost all (97%) of public sector partnerships focus on early childhood care, mental health and substance use, and education. Most of the public-private sector partnerships are with advocacy groups, parenting organizations and family support networks, and community-based coalitions.
ASTHO concludes based on the survey results that health agencies with strong ACEs partnerships have higher capacity in other areas. It reports that agencies with high capacity for public sector partnerships are significantly more likely to have high capacity to: establish leadership presence across three or more sectors; ensure that agency leaders are represented at all levels of government; secure funding sources to prevent ACEs; direct scope of funding to prevent specific ACEs; conduct a needs assessment for ACEs; and share ACEs data.
ASTHO concludes that “Infrastructure qualities, such as managing external and internal partnerships, may indicate the capacity to coordinate other infrastructure aspects, such as increasing leadership buy-in, managing resources, and utilizing data for action.”
The survey found that less than half of agencies practice coordination across multiple strategic plans and include sustainability activities in strategic plans. A higher percentage (60%) of agencies incorporate ACEs or child abuse and neglect into state improvement plans. ASTHO found that “Health agencies with a strategic plan for early child development are significantly more likely to have a high capacity to manage private-sector partnerships.”
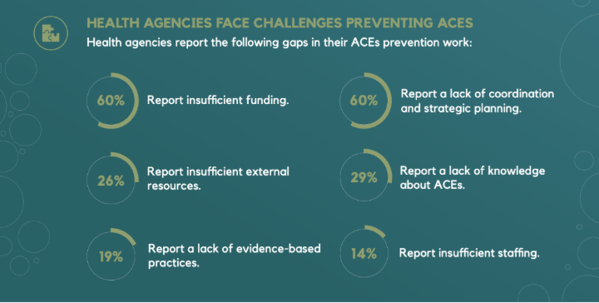
Health agencies report gaps in ACEs prevention work based on:
—insufficient funding (60%)
— lack of coordination and strategic planning (60%)
—insufficient external resources (26%)
—lack of knowledge about ACEs (29%)
—lack of evidence-based practices (19%)
—insufficient staffing (14%)
Looking forward: Health agencies indicate a lack of resources (47%) and lack of knowledge (21%) as some of the challenges they face in addressing ACEs partnership gaps. Given this information, health agencies should review partnerships and strategic plans to understand roles and responsibilities, enhance coordination, maximize resources, navigate “turf wars” in partnerships, and reveal opportunities to maximize resources through braiding and layer funding.
CONCLUSION
The importance of ASTHO’s and CDC’s work to prevent ACEs has only increased during the pandemic. ASTHO addresses this topic directly in its brief “Preventing ACEs During COVID-19.” Additionally, the work of CDC and ASTHO with the PACE-Data2A grants hold the promise of advancing ACEs prevention in the four grantee states and states across the country that are grappling with both the challenges and opportunities presented by the pandemic and the racial reckoning our nation are now experiencing.



Comments (0)